Calvin Chan, Viknesh Sounderajah, Amish Acharya, Pasha Normahani, Colin Bicknell, Celia Riga
|
Abstract Wearable devices and telemonitoring are becoming increasingly widespread in the clinical environment and have many applications in the tracking and maintenance of patient wellbeing. Interventions incorporating these technologies have been used with some success in patients with vascular disorders. Wearable fitness monitors and telemonitoring have been used in the community to mobilise patients with peripheral vascular disease with good results. Additionally, wearable monitors and telemonitoring have been studied for blood pressure monitoring in patients with hypertension. Telemonitoring interventions incorporating electronic medication trays and ingestible sensors have also been found to increase drug adherence in hypertensive patients and ultimately improve health outcomes. However, wearable and telemonitoring interventions often face problems with patient adherence, digital literacy and infrastructure. Further work needs to address these challenges and validate the technology before widespread implementation can occur.
Keywords: Peripheral vascular disease, wearable technology, personalised medicine, telemedicine, digital health
Disclosure: The authors have no conflicts of interest to declare.
Received: Accepted: Published online:
Correspondence Details: Viknesh Sounderajah, Department of Surgery and Cancer, Imperial College London, London W2 1NY, UK. E: vs1108@imperial.ac.uk
Open Access: This work is open access under the CC-BY-NC 4.0 License which allows users to copy, redistribute and make derivative works for non-commercial purposes, provided the original work is cited correctly.
|
Wearable technology refers to the broad category of compact electronic devices that can be incorporated into clothing or accessories.1 These devices are used in the clinical and non-clinical environment and they offer multiple applications that help maintain physiological and psychological wellbeing.2 Wearable technologies not only facilitate self-tracking for the consumer but also allows for remote monitoring and analysis by a third party, such as a healthcare provider.
The Internet of Things is a network of real-world objects that have the ability to communicate data and sense the status of each object and the surrounding environment.3 Through the combined use of wearable devices and Internet of Things technology, patients and healthcare providers may be able to track, monitor and analyse various clinically relevant measurements. This could lead to real-time monitoring of disease progression as well as treatment adherence.
This concept feeds into the premise of telemonitoring, which is defined as the use of telecommunication devices to remotely monitor patients at a distance.4 Of note, telemonitoring is broadly synonymous with biotelemetry, which involves the transmission of health data from one location to another where the data can be interpreted and used to affect healthcare decision-making.4,5 Telemonitoring is useful in collecting biological, environmental or physiological data in a remote setting when direct observation is not possible.5 Common clinically pertinent measurements such as blood pressure (BP), blood glucose and lung function have been successfully tracked using telemonitoring technologies.6–10 The use of telemonitoring allows patients to be managed at home, thereby helping to overcome barriers concerning access to healthcare, such as travel, time and costs.
These technological advancements may prove useful in the management of cardiovascular disease (CVD). CVD is a major global health burden and accounts for a significant proportion of hospital admissions, as well as up to one-third of all deaths globally.11 However, given the importance of conservative management and lifestyle modifications, wearable technology may be able to disrupt the way in which medical therapy and lifestyle modification advice is delivered to this patient cohort. Therefore, in this review, we aim to summarise the current applications of wearable and telemonitoring technologies in facilitating the management of CVD outside the hospital setting.
Current Wearable Technologies
The broad definition of wearable technologies encompasses a variety of devices, such as head-mounted displays, clothing with smart technology, fitness trackers, smart watches and biosensors.
Fitness trackers (activity monitors) allow the long-term daily monitoring of physical activity in a real-world setting and usually take the form of wrist bands, ankle bracelets or clip-ons. Fitness trackers use sensors (pedometers or accelerometers) to detect movement and are therefore able to measure physical activity. Electronic displays on devices allow quick and easy viewing of exercise progress and goals. Many devices are able to transfer data to computer or smartphone apps, allowing remote access to data.
Luley et al. used AiperMotion 440 (Aipermon) fitness trackers as part of an intervention to increase physical activity in patients with metabolic syndrome and found significant improvements in weight loss and markers of the metabolic syndrome.12 In a randomised controlled trial, Frederix et al. used triaxial accelerometers (Yorbody) to monitor physical activity and set daily step-count prescriptions for patients with coronary artery disease enrolled in hospital-based cardiac rehabilitation.13 This study found a significant improvement in lung function assessments and a trend towards fewer rehospitalisations in the intervention group. Kirk et al. conducted a meta-analysis examining the use of wearable devices to alter physical activity behaviour in adults with chronic cardiometabolic disease and found a positive impact on physical health.14
Smart watches have many of the same functions as smartphones, such as mobile applications, internet connectivity and GPS.15 Similar to fitness trackers, smart watches can also incorporate movement and exercise sensing functions, but their functionality is expanding. For example the Apple Watch (Apple) is currently being validated by clinical trials for detection of AF and other abnormal heart rhythms.16
Wearable biosensors are attached to the body for long continuous periods of time and have diagnostic and monitoring applications. The Wearable Biosensor (Philips Medical Systems) is a lightweight, wireless self-adhesive biosensor that can detect vital signs – ECG, respiratory rate, skin temperature – and movement data – posture, fall detection, step count. A study conducted by Braem et al. found that the use of this wearable device as a tool for screening activity levels in patients undergoing transcatheter aortic valve implantation was feasible, but noted some concerns regarding the reliability of the data collection.17 Continuous glucose monitoring can provide real-time blood glucose data otherwise unobtainable by conventional intermittent sampling. GlucoWatch (Cygnus) is a non-invasive wearable continuous glucose monitor that extracts and samples glucose through intact skin via reverse iontophoresis.18 A validation study by Tierney et al. found blood glucose readings from the device were clinically acceptable. However, a randomised trial by Chase et al. found no improvement in glycaemic control with the GlucoWatch, which was, in part, attributed to poor device adherence due to skin irritation.18,19
Peripheral Artery Disease Management
Wearable devices with the ability to monitor movement may be particularly useful in the management of patients with peripheral artery disease (PAD). PAD is a debilitating condition that results in significant walking impairment and poor quality of life.20 Current recommended first-line management for PAD is supervised exercise therapy, with patient mobilisation crucial to prevent disease progression and reduce hospital admissions.21,22 Despite this, patients often face challenges in accessing therapy due to cost, travel and time constraints. This contributes to the low uptake and adherence with such programmes.23,24
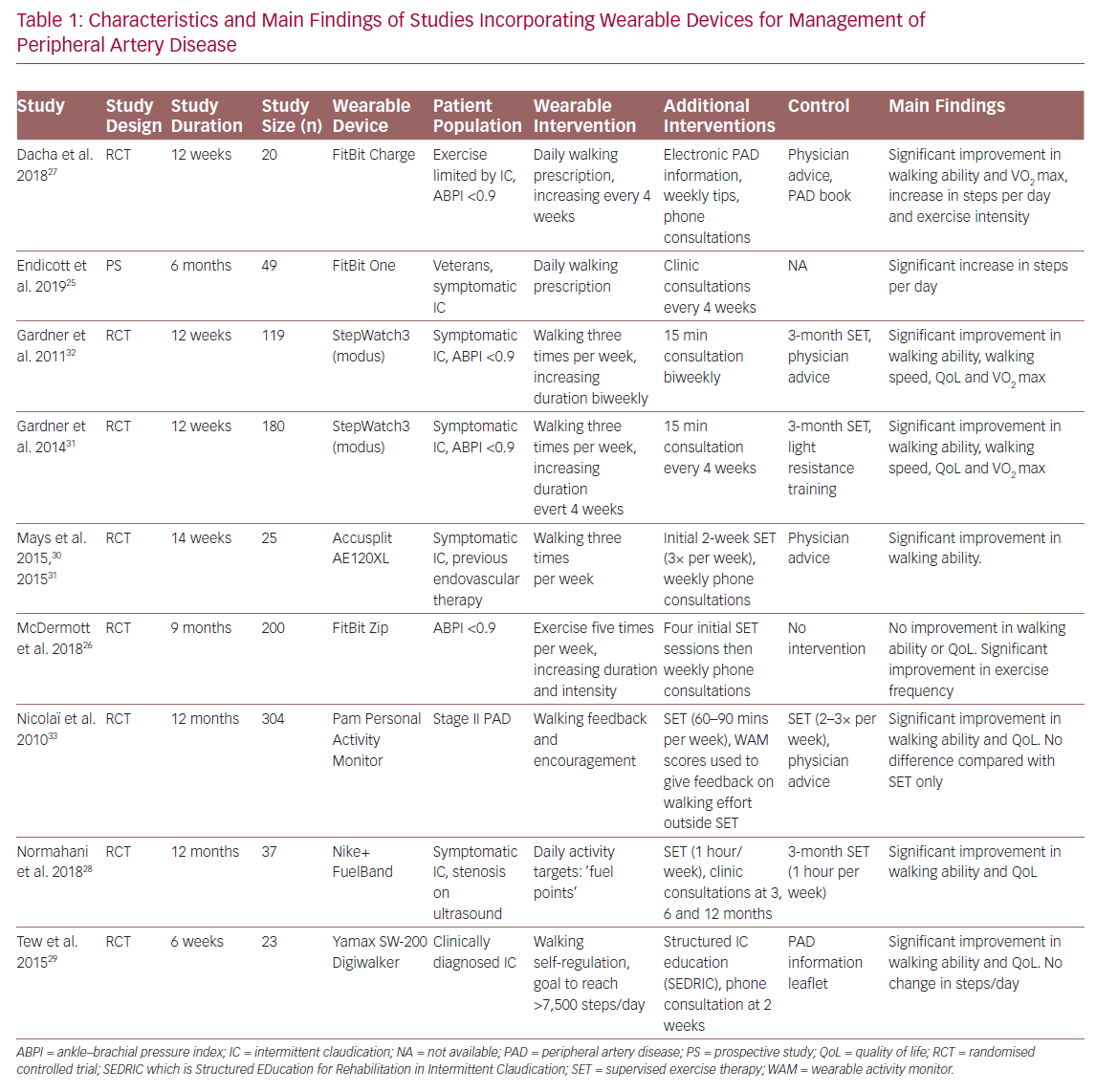
Several studies have investigated the efficacy of home-based exercise programmes incorporating fitness trackers and telemonitoring as an alternative to supervised exercise (Table 1).25–33 Duscha et al. used wrist-worn commercially available fitness trackers (FitBit Charge, FitBit) to monitor daily physical activity and set exercise prescriptions based increasing patients’ step count each day.27 Patients wore fitness trackers continuously during waking hours and daily step count was synchronised with smartphones where it could be remotely viewed. This allowed investigators to not only monitor physical activity, but also offer personalised feedback via phone calls. Patients using the fitness tracker intervention were found to have significant improvement in claudication distance, maximum walking distance and steps walked per day, compared with baseline.
Similarly, Normahani et al. incorporated the Nike+ FuelBand (Nike) fitness tracker as part of a home-based exercise intervention for patients with PAD.28 Instead of setting exercise prescriptions using step count, ‘fuel points’ were used, which measure overall activity and movement. Online accounts on the Nike+ website allowed activity data to be reviewed at follow-up visits and exercise prescriptions could be programmed into patient devices. The study found significant increases in walking ability and quality of life in patients using the device, compared with those attending a weekly 1-hour supervised exercise session over a 12-month period.
In addition to using the AE120XL pedometer (Accusplit) to track daily physical activity and weekly phone consultations, Mays et al. incorporated an element of coaching into their study.30 This allowed them to identify local barriers and encourage exercise adherence. This involved an assessment of a patient’s local area using Google Street View to identify walking routes and community resources, such as benches on which to rest. Moreover, they identified potential barriers to walking, such as discontinuous pavements.30,34 This resulted in significant improvements in walking ability for the intervention group compared with baseline and usual care.
The use of smartphone applications may also be beneficial for the remote monitoring and management of PAD. Ata et al. developed VascTrac, an Apple smartphone app that enabled remote collection of medical and physical activity data.35 VascTrac is able to record measures of daily physical activity (steps walked, distance walked, flights of stairs climbed and maximum continuous number of steps) using the built-in accelerometer in Apple smartphones. Patients were sent notifications through the app to perform twice-weekly 6-minute walk tests which allows tracking of changes in walking ability. Study results are yet to be published.
Blood Pressure Monitoring
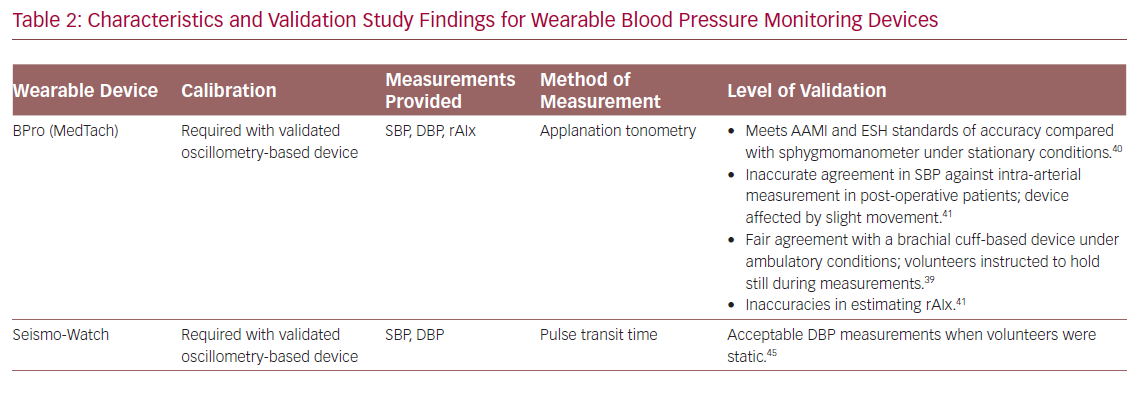
Hypertension is a well-known risk factor for CVD.21 Environmental factors can often limit the usefulness of conventional BP measurements because of phenomena such as white-coat, masked and nocturnal hypertension.36 Home measurement is a superior method of determining BP and wearable devices are well established for this purpose.37 Apart from traditional oscillometry-based BP measurement (involving an inflatable cuff), wearable devices also use other non-invasive methods of eliciting measures of BP such as tonometry, volume clamp, pulse wave velocity and pulse transit time (Table 2).38
The BPro (Healthstats) is a cuffless, wrist-bound BP measurement system that works via arterial applanation tonometry. The wrist monitor incorporates a small protruding force sensor that rests over the radial artery and captures the arterial pulse waveform.39 The device requires initial calibration to bronchial BP using a standard oscillometry-based BP monitor. In a validation study, the device was found to meet the accuracy criteria for systolic and diastolic BP in both European Society of Hypertension protocol and Association for the Advancement of Medical Instrumentation (AAMI) standards under stationary conditions.40 However, in a study comparing accuracy of the BPro against intra-arterial BP measurement in post-operative patients, there were significant inaccuracies according to AAMI standards in systolic and mean BP between the methods, which was attributed to patient movement.41 A 24-hour study comparing the BPro to conventional arm-bound oscillometry-based BP monitoring in 50 normotensive and prehypertensive volunteers found fair agreement between the two devices.39 However, during BP measurements the volunteers were asked to keep still and the BPro was unable to obtain almost 50% of the scheduled measurements.39
Characteristics and Main Findings of Studies Incorporating Wearable Devices
Characteristics and Validation Study Findings for Wearable Blood Pressure Monitoring Devices
Characteristics and Validation Study Findings for Wearable Blood Pressure Monitoring Devices
In addition to BP measurement, radial augmentation index (rAIx) can be calculated from radial wave pulse measurements from the BPro.42 The rAIx has been proposed as an estimate of central BP and a useful parameter of vascular function and ageing.43 Although there were discrepancies in rAIx measured by BPro versus a reference device, Vardoulis et al. developed and validated a novel wrist-bound tonometer that produced accurate rAIx readings compared with a reference hand-held tonometer.42,44
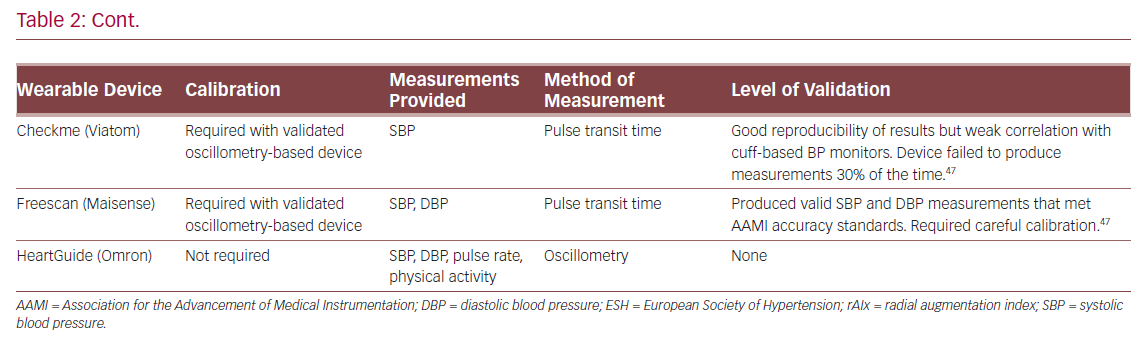
The SeismoWatch is an example of a wrist-worn BP monitor that functions via pulse transit time.45 To obtain BP measurements, the watch face contains an accelerometer which is pressed for a short duration on the sternum to obtain a seismocardiogram and determine timing of left ventricular ejection. This is compared with a distal reading from a wrist-obtained photoplethysmogram to obtain the pulse transit time and, therefore, an estimate of BP.45 In a small feasibility study, the device was found to obtain acceptable mean and diastolic BP, but required subjects to perform measurements while static.45 Similarly, Ogink et al. investigated the feasibility of a cuffless BP monitor (Checkme Pro, Viatom) based on pulse transit time to measure systolic BP of hypertensive patients at home.46 The study found that the device produced reproducible BP readings and had good adherence due to its ease of use. However, the device was limited by its inability to measure diastolic BP and failure to measure BP 30% of the time.
Boubouchairopoulou et al. validated a cuffless BP monitor (FreeScan, Maisense) that obtained readings via pulse transit time.47 In large successive feasibility and validation studies (a total of 313 patients were involved in the four feasibility studies), the device was found capable of obtaining systolic and diastolic BP readings when compared with a standard mercury sphygmomanometer. However, accurate readings required a device sensor upgrade and careful initial device calibration in a research setting. Further work is needed to investigate the validity of this prototype device in a clinical setting.
The HeartGuide (Omron Corp) is a novel smartwatch with the ability to monitor BP.48 It uses the traditional oscillometry-based principle where the strap of the wrist-worn device acts as a BP cuff and allows BP measurement for up to 7 days on a single charge. It has additional abilities such as data synchronisation to an online account as well as step count and heart rate monitoring. However, this device is yet to be validated.
Best Medical Therapy Compliance Monitoring
Non-adherence to medication in hypertensive patients is a contributing factor to poor BP control and is associated with higher risks of vascular events, hospitalisation and increased healthcare costs.49 Davidson et al. developed and validated a telemonitoring intervention involving electronic medication trays, Bluetooth-enabled BP monitors and SMS messaging.50 The electronic medication tray (Maya, MedMinder) reminded patients to take their dose at the prescribed time first with a blinking light, then a 30-minute chime and finally an automated phone call or SMS. Patients were reminded to use the Bluetooth-enabled BP monitor (UA-767PlusBT, A&D Engineering) via SMS, and readings were sent from the device to a provided smartphone and a remote data repository via cellular network. If BP measurements were above a predefined threshold, patients were instructed via phone to obtain additional measurements and their physician was alerted. Patients in the telemonitoring group had significant lower systolic and diastolic BP across the study’s duration and a significantly greater proportion achieved BP control.
Frias et al. validated a system involving ingestible sensors and wearable sensor patches (Proteus Discover, Proteus Digital Health) for patients with uncontrolled hypertension and type 2 diabetes.51 The medications of patients in the intervention group were co-encapsulated with ingestible sensors. Once swallowed, the ingestible sensor would activate and send a signal to the adhesive sensor patch. Data from the patch was then transmitted to an online data repository via a smartphone app. Data could be viewed by patients on the mobile app and remotely by their physicians. The mobile app also prompted patients to take their medications at the prescribed times. There were significant improvements in systolic BP and a larger proportion of patients achieved their BP goal in the intervention group. In terms of diabetes, however, there was no significant difference in HbA1c or fasting plasma glucose between intervention and control groups. Physicians with access to the online data made approximately three times more medical decisions per participant and patients with uncontrolled hypertension in the intervention group were more likely to be given a medication adjustment or adherence counselling. However, a comparison of adherence to medication could not be assessed due to the intrinsic design of the study.
Discussion
The NHS Long Term Plan pushes for a digital transformation where digitally enabled care will become mainstream.52 As the NHS shifts towards a digital-first approach for patient consultations, there must be robust and validated methods for remote patient monitoring to aid analysis and decision-making by clinicians. Concurrently, wearable technologies are increasingly ubiquitous, with an estimated 722 million devices connected to the internet.48,49 These trends are set to continue, with shipments of wearable devices expected to almost double from 2019 to 2022, increasing from 226 million to 453.19 million.53 As these technologies become more widespread, clinicians have the responsibility to be early adopters, harnessing the potential they possess especially regarding their telemonitoring properties. However, before these technologies can be implemented clinically, a number of issues must first be addressed.
Compliance and the Digital Divide
The digital divide is the difference between those who possess technological skills and those who do not.54 Cardiovascular diseases most commonly manifest in older patients, the cohort with the lowest rates of smartphone adoption and digital literacy.55 It has been suggested that older adults are reluctant to use mobile electronic devices due to factors such as lack of knowledge, disinterest or vision impairment.56 This potentially limits the use of wearable technology in this population.
Poor adherence has also been demonstrated in other groups. Several studies included in this review mentioned limitations of technology due to know-how or non-use. Ogink et al. found that only 36% of participants correctly performed BP measurements with their cuffless monitor after instruction.46 However, the authors suggested that education using a set procedure or an instructional video may increase correct usage.46,57,58 Nicolaï et al. found that 30% of patients in the wearable intervention group did not use the prescribed fitness tracker for the duration of the study or at all.33 Similarly, Endicott et al. reported 43% non-use of fitness trackers by participants.25 Although adherence to the use of fitness trackers was very good (>80%) in a series of trials by Gardner et al., it was noted that participants were volunteers.31,32 This exposes the study to selection bias, where patients who were more comfortable with technology or were more motivated were more likely to participate.
Further work is needed to determine digital literacy in vascular patients. This could be achieved through validated literacy questionnaires such as eHEALS for eHealth literacy or MDPQ-16 for mobile device proficiency.59,60 Thus, appropriate wearable and telemonitoring interventions may be used and adequate coaching given to participants.
Digital Infrastructure
The expansion of wearable and telemonitoring interventions is limited by infrastructure. Hovey et al. investigated several practical aspects that negatively affected telemonitoring.61 Suboptimal internet connectivity, especially in rural areas, affected data collection and patient adherence. There were hardware issues that needed to be diagnosed remotely and required replacement equipment, thereby reducing patient access and increasing costs. Software issues were identified that could affect large-scale implementations of telemonitoring. For successful wearable and telemonitoring interventions, there is a need for robust and reliable infrastructure. Larger-scale extended studies could be conducted to validate the large-scale extension of a wearable or telemonitoring intervention.
Cost
The up-front cost of novel technology is often cited as prohibitive to widespread adoption. In fact, wearable and telemonitoring interventions may have cost benefits compared with conventional management. With regards to PAD management, a standard 3-month supervised exercise programme was estimated to cost about £235–£345 per patient in a 2013 study.62 In comparison, fitness trackers can cost as little as £21 per unit, although this can be considerably higher with more advanced devices. Furthermore, this cost can be offset by the reduction in travel expenses for the patient. These interventions additionally allow the individual tailoring of exercise requirements for each patient, which cannot be achieved with group supervised exercise.
Similarly, telemonitoring hypertension interventions may be cost-efficient. Low adherence to antihypertensive therapy was estimated to cost US$3,574 per patient over a 3-year period.49 In a 2015 study, Davidson et al. estimated the cost of their telemonitoring intervention (electronic medication tray, SMS encouragement, Bluetooth BP monitor and associated support staff) to be US$65 per month for patients who owned a smartphone and US$128 per month for those who did not.50 Investigators noted that the average cost of an emergency department visit to be US$5,923 and the intervention group had a 57% reduction in visits compared with those receiving standard care, therefore giving a US$17,548 cost saving over a 6-month period. In addition, as telemonitoring can potentially identify patients with white-coat hypertension. It may avoid overtreatment and associated medication costs.7 There is a need, however, for further work to formally evaluate cost-effectiveness of wearable and telemonitoring interventions in cardiovascular patients.
Conclusion
Wearable technologies are becoming increasingly prevalent and there is some evidence that wearable and telemonitoring interventions may be beneficial for managing vascular patients and keeping them out of hospital. With healthcare moving towards a digital future, it is inevitable that wearable devices and telemonitoring will become increasingly widespread in the clinical environment. More work is needed to validate these technologies with regards to digital literacy of patients, cost-effectiveness and supporting digital infrastructure before widespread implementation.
- Tehrani K, Michael A. Wearable technology and wearable devices: everything you need to know. Wearable Devices Magazine 2014. http://www.wearabledevices.com/what-is-a-wearable-device (accessed 10 March 2020).
- Iqbal MH, Aydin A, Brunckhorst O, et al. A review of wearable technology in medicine. J R Soc Med 2016;109:372–80. Crossref| PubMed
- Haghi M, Thurow K, Stoll R. Wearable devices in medical internet of things: Scientific research and commercially available devices. Healthc Inform Res 2017;23:4–15. Crossref| PubMed
- Meystre S. The current state of telemonitoring: A comment on the literature. Telemed J E Health 2005;11:63–9. Crossref| PubMed
- Güler NF, Übeyli ED. Theory and applications of biotelemetry. J Med Syst 2002;26:159–78. Crossref| PubMed
- Artinian NT, Flack JM, Nordstrom CK, et al. Effects of nurse-managed telemonitoring on blood pressure at 12-month follow-up among urban African Americans. Nurs Res 2007;56:312–22. Crossref| PubMed
- Artinian NT, Washington OGM, Templin TN. Effects of home telemonitoring and community-based monitoring on blood pressure control in urban African Americans: A pilot study. Hear Lung 2001;30:191–9. Crossref| PubMed
- Gómez EJ, Hernando ME, García A, et al. Telemedicine as a tool for intensive management of diabetes: the DIABTel experience. Comput Methods Programs Biomed 2002;69:163–77. Crossref| PubMed
- Montori VM, Helgemoe PK, Guyatt GH, et al. Telecare for patients with type 1 diabetes and inadequate glycemic control: a randomized controlled trial and meta-analysis. Diabetes Care 2004;27:1088–94. Crossref| PubMed
- Finkelstein J, Cabrera MR, Hripcsak G. Internet-based home asthma telemonitoring: Can patients handle the technology? Chest 2000;117:148–55. Crossref| PubMed
- Roth GA, Johnson C, Abajobir A, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol 2017;70:1–25. Crossref| PubMed
- Luley C, Blaik A, Götz A, et al. Weight loss by telemonitoring of nutrition and physical activity in patients with metabolic syndrome for 1 year. J Am Coll Nutr 2014;33:363–74. Crossref| PubMed
- Frederix I, Driessche N Van, Hansen D, et al. Increasing the medium-term clinical benefits of hospital-based cardiac rehabilitation by physical activity telemonitoring in coronary artery disease patients. Eur J Prev Cardiol 2015;22:150–8. Crossref| PubMed
- Kirk MA, Amiri M, Pirbaglou M, et al. Wearable technology and physical activity behavior change in adults with chronic cardiometabolic disease: a systematic review and meta-analysis. Am J Health Promot 2019;33:778–91. Crossref| PubMed
- Wright R, Keith L. Wearable technology: if the tech fits, wear it. Journal of Electronic Resources in Medical Libraries 2014;11:204–16. Crossref
- Turakhia MP, Desai M, Hedlin H, et al. Rationale and design of a large-scale, app-based study to identify cardiac arrhythmias using a smartwatch: the Apple Heart Study. Am Heart J 2019;207:66–75. Crossref| PubMed
- Braem CIR. The Philips wearable biosensor in transcatheter aortic valve implantation treatment workflow. Usability and feasibility of the wearable biosensor. MSc Thesis. University of Twente. Enschede, the Netherlands, 2019. https://essay.utwente.nl/77157/ (accessed 10 March 2020).
- Tierney MJ, Tamada JA, Potts RO, et al. Clinical evaluation of the GlucoWatch® biographer: a continual, non-invasive glucose monitor for patients with diabetes. Biosens Bioelectron 2001;16:621–9. Crossref| PubMed
- Chase HP. A randomized multicenter trial comparing the glucowatch biographer with standard glucose monitoring in children with type 1 diabetes. Diabetes Care 2005;28:1101–6. Crossref| PubMed
- Spronk S, White JV, Bosch JL, et al. Impact of claudication and its treatment on quality of life. Semin Vasc Surg 2007;20:3–9. Crossref| PubMed
- Aboyans V, Ricco JB, Bartelink MLEL, et al. 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS): document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal. Eur Heart J 2017;39:763–816. Crossref| PubMed
- Weitz JI, Byrne J, Clagett GP, et al. Diagnosis and treatment of chronic arterial insufficiency of the lower extremities: a critical review. Circulation 1996;94:3026–49. Crossref| PubMed
- Harwood AE, Smith GE, Cayton T, et al. A systematic review of the uptake and adherence rates to supervised exercise programs in patients with intermittent claudication. Ann Vasc Surg 2016;34:280–9. Crossref| PubMed
- Shalhoub J, Hamish M, Davies AH. Supervised exercise for intermittent claudication – an under-utilised tool. Ann R Coll Surg Engl 2009;91:473–6. Crossref| PubMed
- Endicott KM, Hynes CF, Amdur R, et al. A modified activity protocol for claudication. J Cardiovasc Surg (Torino) 2019;60:382–7. Crossref| PubMed
- McDermott MM, Spring B, Berger JS, et al. Effect of a home-based exercise intervention of wearable technology and telephone coaching on walking performance in peripheral artery disease: the HONOR randomized clinical trial. JAMA 2018;319:1665–76. Crossref| PubMed
- Duscha BD, Piner LW, Patel MP, et al. Effects of a 12-week mHealth program on functional capacity and physical activity in patients with peripheral artery disease. Am J Cardiol 2018;122:879–84. Crossref| PubMed
- Normahani P, Kwasnicki R, Bicknell C, et al. Wearable sensor technology efficacy in peripheral vascular disease (wSTEP): a randomized controlled trial. Ann Surg 2018;268:1113–8. Crossref| PubMed
- Tew GA, Humphreys L, Crank H, et al. The development and pilot randomised controlled trial of a group education programme for promoting walking in people with intermittent claudication. Vasc Med 2015;20:348–57. Crossref| PubMed
- Mays RJ, Hiatt WR, Casserly IP, et al. Community-based walking exercise for peripheral artery disease: An exploratory pilot study. Vasc Med 2015;20:339–47. Crossref| PubMed
- Gardner AW, Parker DE, Montgomery PS, et al. Step-monitored home exercise improves ambulation, vascular function, and inflammation in symptomatic patients with peripheral artery disease: a randomized controlled trial. J Am Heart Assoc 2014;3:e001107. Crossref| PubMed
- Gardner AW, Parker DE, Montgomery PS, et al. Efficacy of quantified home-based exercise and supervised exercise in patients with intermittent claudication: a randomized controlled trial. Circulation 2011;123:491–8. Crossref| PubMed
- Nicolaï SPA, Teijink JAW, Prins MH, et al. Multicenter randomized clinical trial of supervised exercise therapy with or without feedback versus walking advice for intermittent claudication. J Vasc Surg 2010;52:348–55. Crossref| PubMed
- Rundle AG, Bader MDM, Richards CA, et al. Using google street view to audit neighborhood environments. Am J Prev Med 2011;40:94–100. Crossref| PubMed
- Ata R, Gandhi N, Rasmussen H, et al. IP225 VascTrac: a study of peripheral artery disease via smartphones to improve remote disease monitoring and postoperative surveillance. J Vas Surg 2017;65:115S–6. Crossref
- O’Brien E, Parati G, Stergiou G, et al. European Society of Hypertension position paper on ambulatory blood pressure monitoring. J Hypertens 2013;31:1731–68. Crossref| PubMed
- Parati G, Stergiou GS, Asmar R, et al. European Society of Hypertension Practice guidelines for home blood pressure monitoring. J Hum Hypertens 2010;24:779–85. Crossref| PubMed
- Peter L, Noury N, Cerny M. A review of methods for non-invasive and continuous blood pressure monitoring: pulse transit time method is promising? IRBM 2014;35:271–82. Crossref
- Komori T, Eguchi K, Hoshide S, et al. Comparison of wrist-type and arm-type 24-h blood pressure monitoring devices for ambulatory use. Blood Press Monit 2013;18:57–62. Crossref| PubMed
- Nair D, Tan SY, Gan HW, et al. The use of ambulatory tonometric radial arterial wave capture to measure ambulatory blood pressure: the validation of a novel wrist-bound device in adults. J Hum Hypertens 2008;22:220–2. Crossref| PubMed
- Harju J, Vehkaoja A, Kumpulainen P, et al. Comparison of non-invasive blood pressure monitoring using modified arterial applanation tonometry with intra-arterial measurement. J Clin Monit Comput 2018;32:13–22. Crossref| PubMed
- Garcia-Ortiz L, Recio-Rodríguez JI, Canales-Reina JJ, et al. Comparison of two measuring instruments, B-pro and SphygmoCor system as reference, to evaluate central systolic blood pressure and radial augmentation index. Hypertens Res 2012;35:617–23. Crossref| PubMed
- Kohara K, Tabara Y, Oshiumi A, et al. Radial augmentation index: A useful and easily obtainable parameter for vascular aging. Am J Hypertens 2005;18(1 Suppl):11–4. Crossref| PubMed
- Vardoulis O, Saponas TS, Morris D, et al. In vivo evaluation of a novel, wrist-mounted arterial pressure sensing device versus the traditional hand-held tonometer. Med Eng Phys 2016;38:1063–9. Crossref| PubMed
- Carek AM, Conant J, Joshi A, et al. SeismoWatch: wearable cuffless blood pressure monitoring using pulse transit time. Proc ACM Interact Mob Wearable Ubiquitous Technol 2017;1:40. Crossref| PubMed
- Ogink PA, de Jong JM, Koeneman M, et al. Feasibility of a new cuffless device for ambulatory blood pressure measurement in patients with hypertension: mixed methods study. J Med Internet Res 2019;21:e11164. Crossref| PubMed
- Boubouchairopoulou N, Kollias A, Chiu B, et al. A novel cuffless device for self-measurement of blood pressure: Concept, performance and clinical validation. J Hum Hypertens 2017;31:479–82. Crossref| PubMed
- Arakawa T. Recent research and developing trends of wearable sensors for detecting blood pressure. Sensors (Switzerland) 2018;18:e2772. Crossref| PubMed
- Dragomir A, Côté R, Roy L, et al. Impact of adherence to antihypertensive agents on clinical outcomes and hospitalization costs. Med Care 2010;48:418–25. Crossref| PubMed
- Davidson TM, McGillicuddy J, Mueller M, et al. Evaluation of an mHealth medication regimen self-management program for African American and Hispanic uncontrolled hypertensives. J Pers Med 2015;5:389–405. Crossref| PubMed
- Frias J, Virdi N, Raja P, et al. Effectiveness of digital medicines to improve clinical outcomes in patients with uncontrolled hypertension and type 2 diabetes: Prospective, open-label, cluster-randomized pilot clinical trial. J Med Internet Res 2017;19:e246. Crossref| PubMed
- NHS England. Digitally-enabled care will go mainstream across the NHS. In: The NHS Long Term Plan. NHS England; 2018. https://www.longtermplan.nhs.uk/online-version/chapter-5-digitally-enabl… (accessed 10 March 2020).
- Forecast unit shipments of wearable devices worldwide from 2017 to 2019 and in 2022 (in million units), by category. Statista; 2018. https://www.statista.com/statistics/385658/electronic-wearable-fitness-d… (accessed 10 March 2020).
- Blau A. Access isn’t enough: merely connecting people and computers won’t close the digital divide. American Libraries 2002;33:50–2.
- Berenguer A, Goncalves J, Hosio S, et al. Are smartphones ubiquitous? An in-depth survey of smartphone adoption by seniors. IEEE Consumer Electronics Magazine 2017;6:104–10. Crossref
- Mohadisdudis HM, Ali NM. A study of smartphone usage and barriers among the elderly. Presented at 3rd International Conference on User Science and Engineering (i-USEr). Institute of Electrical and Electronics Engineers Shah Alam, Malaysia, 2–5 September 2014. Crossref
- Bonderup AM, Hangaard SV, Lilholt PH, et al. Patient support ICT tool for hypertension monitoring. Stud Health Technol Inform 2012;180:189–93. Crossref| PubMed
- Mengden T, Chamontin B, Phong Chau N, et al. User procedure for self-measurement of blood pressure. First International Consensus Conference on Self Blood Pressure Measurement. Blood Press Monit 2000;5:111–29. PubMed
- Roque NA, Boot WR. A new tool for assessing mobile device proficiency in older adults: the mobile device proficiency questionnaire. J Appl Gerontol 2018;37:131–56. Crossref| PubMed
- van der Vaart R, van Deursen AJ, Drossaert CHC, et al. Does the eHealth literacy scale (eHEALS) measure what it intends to measure? Validation of a Dutch version of the eHEALS in two adult populations. J Med Internet Res 2011;13:e86. Crossref| PubMed
- Hovey L, Kaylor MB, Alwan M, et al. Community-based telemonitoring for hypertension management: Practical challenges and potential solutions. Telemed e-Health 2011;17:645–51. Crossref| PubMed
- Bermingham SL, Sparrow K, Mullis R, et al. The cost-effectiveness of supervised exercise for the treatment of intermittent claudication. Eur J Vasc Endovasc Surg 2013;46:707–14. Crossref| PubMed