Nolan Mann, Hosam El Sayed, Jean Panneton
|
Abstract Endovascular treatment has become an accepted method in the treatment of aortoiliac occlusive disease. Bare metal stents have been used in the treatment of aortoiliac disease since the early 1990s. More recently, the use of covered stent grafts in the aortoiliac segment has shown clinical benefit in terms of patency, freedom from reintervention and quality of life. The VBX FLEX study evaluated the safety and efficacy of the Gore VBX stent graft for use in the aortoiliac segment. The early and mid-term data on the Gore VBX stent graft have shown it to be a safe device for use in the treatment of aortoiliac occlusive disease. This review examines the use of stents in aortoiliac occlusive disease with specific focus on the VBX FLEX Study. Keywords: Aortoiliac occlusive disease, common iliac stent, covered stent, balloon expandable, VBX, VBX FLEX study Disclosure: JP is a consultant for WL Gore and Getinge. All other authors have no conflicts of interest to declare. Received: 07 September Accepted: 11 January 2022Published online: 11 April 2022 Citation: Vascular & Endovascular Review 2022;5:e03. DOI:https://doi.org/10.15420/ver.2021.12 Correspondence Details: Jean M Panneton, EVMS Division of Vascular Surgery, Sentara Heart Hospital, 600 Gresham Drive, Suite 8620, Norfolk, VA 23507, US. E: PannetJM@EVMS.edu
Open Access:
This work is open access under the CC-BY-NC 4.0 License which allows users to copy, redistribute and make derivative works for non-commercial purposes, provided the original work is cited correctly.
|
Advances in endovascular techniques and technology have allowed the treatment of more extensive iliac lesions, and current endovascular treatment of AIOD often involves primary stenting unilaterally or the use of kissing iliac stents for disease involving the aortic bifurcation.
Evolution of Endovascular Treatment of the Iliac Segment
Endovascular treatment of the iliac segment was largely limited to angioplasty alone through the late 1980s and early 1990s. The first major experience from Palmaz et al. demonstrated both the safety and efficacy of balloon-expandable stent placement in the iliac segment.5–7 This landmark paper laid the foundation for the transition of treatment of the aortoiliac segment from primarily surgical to an endovascular approach.5
Selective Stenting Versus Primary Stenting
Many studies have followed the initial reports of Palmaz et al. and have reiterated favourable results of selective stent placement in lesions refractory to angioplasty alone. The 1998 Dutch Iliac Stent trial was a randomised comparison of primary iliac stenting and selective iliac stenting in the case of residual stenosis after angioplasty in 279 patients.8 The investigators demonstrated equivalent iliac patency at 2 years between the two groups and greater cost efficiency in the selective stenting group. However, the majority of these lesions were TASC A and B, 43% of patients in the selective group required stenting for suboptimal outcome with angioplasty alone, and there was an increased complication rate in the selective stenting group (7% versus 4%).8
In a more recent study, AbuRahma et al. demonstrated superior clinical success with primary stenting over selective stenting in TASC C and D lesions.9 In that study, 110 consecutive patients with 149 iliac lesions underwent primary iliac stenting. These patients were compared to a cohort of 41 patients with 41 iliac lesions who had angioplasty followed by selective stenting if there was a suboptimal percutaneous transluminal angioplasty result. The study found that there was comparable initial and late clinical success in TASC A and B lesions.9 However, in TASC C and D lesions, primary stenting was superior to selective stenting with early clinical success of 93% versus 46% and late clinical success of 84% versus 46%.8 It was also noted that the selective stenting group had a significantly higher rate of perioperative complications than the group undergoing primary stenting (24% versus 2.7%).9 There were 10 complications in the selective stenting group, which included seven cases of early postintervention iliac artery thrombosis, one case of postintervention deep venous thrombosis, one episode of postoperative bleeding requiring surgery and one case of superficial cellulitis.9 In the primary stenting group there were three complications, all of which were minor postintervention haematomas.9
GORE VIABAHN VBX BalloonExpandable Endoprosthesis
A large meta-analysis by Ye et al., in which 16 reports were reviewed with a total of 958 patients, showed a superior primary patency rate for primary stenting compared with selective stenting for TASC C and D aortoiliac lesions.10
The STAG trial randomised 112 patients to primary stenting (n=57) or angioplasty (n=55) for iliac artery occlusion.11 There was a significant difference in the technical success rate between the angioplasty and primary iliac stenting groups (84% versus 98%, respectively).11 In addition, there was a significant difference in the rate of major complications, which was 20% in the angioplasty group compared with 5% in the stenting group.11
Together, the data support the use of primary iliac stenting in the case of more advanced aortoiliac lesions, not only because of its superior technical success and superior early and late clinical outcomes, but also because of the significantly lower complication rates.
Covered Versus Uncovered Iliac Stents
The long-term efficacy of bare metal stents is generally accepted to be limited due to progressive narrowing of the luminal diameter as a result of neointimal hyperplasia. Conversely, covered stents are designed to exclude the diseased vessel wall and prevent in-stent restenosis from intimal hyperplasia, leading to improved long-term patency.
The COBEST trial was a prospective randomised controlled trial including 125 patients with 168 individual iliac artery lesions randomised to receive a covered balloon-expandable stent or a bare metal stent.12 The investigators found that patients treated with covered stents were more likely to remain free of restenosis at 18 months, with a hazard ratio of 0.35. In addition, they noted that this benefit was more significant when using covered stents for TASC C and D aortoiliac lesions.12 Sabri et al. reported similar findings when the placement of comparing bare metal and covered stents for aortic bifurcation disease.13
The COBEST investigators published 5-year durability data in 2016.14 These data indicated that covered stents offered significantly higher patency rates than bare-metal stents at 18, 24, 48 and 60 months (95.1%, 82.1%, 79.9% and 74.7% versus 73.9%, 70.9%, 63% and 62.5%, respectively).14 Patients who received a covered stent also required fewer target limb revascularisations than those who received a bare metal stent and enjoyed sustained improvement in the ankle–brachial index (ABI).14 However, as expected, this did not lead to a significant difference in major amputation rate because most of the patients enrolled in the study were claudicants.14
Results of the ongoing double-blinded, randomised DISCOVER trial are awaited for comparison to the COBEST trial.15
Comparison of Covered Stents for Aortoiliac Segment
The COBEST trial was performed with the Advanta V12 covered stent (Atrium Medical), which is expanded polytetrafluoroethylene (ePTFE) encapsulated and mounted on a non-compliant balloon. This was the first covered balloon-expandable stent with an indication for use in the aortoiliac segment outside the US. There are currently three balloon-expandable covered stents available for the treatment of AIOD in the US: the LifeStream (BD/Bard Peripheral Vascular), the iCAST/Advanta V12 (Getinge) and the Gore VBX (WL Gore and Associates).
The BOLSTER trial evaluated the efficacy of the LifeStream stent.15 This is a balloon-expandable, ePTFE-encapsulated stainless steel stent. The trial results were promising, with primary patency of 89.1% at 9 months and overall improvement in quality of life.16
The iCARUS trial examined the iCAST stent in the aortoiliac segment.17 The iCAST has a similar design to the LifeStream stent, being an ePTFE-encapsulated stainless steel stent. Early results were impressive, with a freedom from target lesion revascularisation (TLR) rate of 97.2% at 9 months and 86.6% at 3 years.17 A sustained clinical improvement was noted in the trial population at the 3-year mark. It is notable that there was a low percentage of TASC C and D lesions (5.8%) in that study.17
The most recent trial, the VBX FLEX study, was an industry-sponsored trial conducted at 26 sites in the US and one site in New Zealand to assess the safety and efficacy of the VBX stent graft for use in AIOD.18 The VBX stent graft is unique in that it is composed of independent stainless steel rings connected by graft material (Figure 1). It is the only peripheral stent graft without longitudinal struts. This allows for increased flexibility while maintaining shape and luminal diameter. The stent also has high radial strength, is resistant to foreshortening, has considerable ability to post dilate and can be accurately placed. The device’s deployment balloon also has an elastomer film that improves device sequestration while tracking, preventing inadvertent stent dislodgement. In addition, the luminal surface has covalent heparin bonding. The results of the initial study were published in 2017.18 The 3-year follow-up outcomes have recently been published.19
VBX FLEX Study Overview
The VBX FLEX study was an industry-sponsored prospective multicentre single-arm clinical trial conducted in the US (26 centres) and New Zealand (one centre) with the intention of evaluating the safety and efficacy of the Gore VBX stent graft for the treatment of iliac lesions.18 Patients with Rutherford Class 2–4 disease with at least one de novo or restenotic target lesion >50% were included. In addition, patients were required to have at least one sufficient (<50% stenosis) infrapopliteal run-off vessel that did not require treatment. Anatomical exclusion criteria included lesions that would require atherectomy to facilitate device delivery or coverage of the internal iliac artery. Between December 2013 and August 2015, 234 stent grafts were implanted in 134 patients (mean age 66 years; 79 men) across 213 lesions. After implantation of the VBX stent graft, patients underwent clinical evaluations that included duplex ultrasound, ABI measurements, Rutherford classification assessments and a walking impairment questionnaire at each follow-up visit at 1, 9, 12, 24 and 36 months.
The primary endpoint of the VBX FLEX study was major adverse events within 30 days, MI within 30 days, TLR within 9 months and amputation above the metatarsals in the treated leg within 9 months. Secondary endpoints were acute procedural success (<30% residual stenosis prior to procedure completion), 30-day clinical success (improvement of at least one Rutherford category at the first follow-up), primary, assisted primary and secondary patency rates at 1 year, freedom from TLR, freedom from clinically driven TLR (CD-TLR), freedom from target vessel revascularisation (TVR), freedom from clinically driven TVR, change in Rutherford category, ABI and functional status at up to 3 years.
VBX FLEX Study Results
Procedural Characteristics
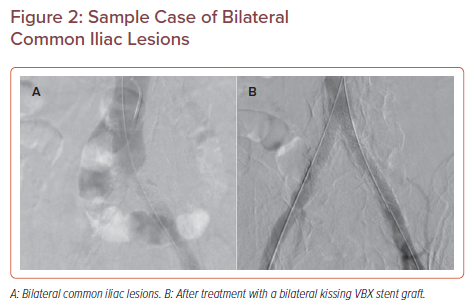
Half the study population received bilateral iliac stents, many of which had aortic bifurcation disease requiring a kissing stent procedure (Figure 2); 15.4% of patients had stents placed in the external iliac artery alone.18 Total occlusions were found in 28 of 210 lesions (13.3%). There was 100% technical success with an overall median change in device length from predeployment to final implantation of −0.05 mm, indicating a high degree of resistance to foreshortening.
Early Results
The primary endpoints of the VBX FLEX study included a 97.7% rate of freedom from TLR within 9 months, a 2.3% major adverse events rate, no MIs, no device or procedure-related deaths and no major amputations within 9 months. The 9-month composite primary endpoint for the overall study population was 2.3% (three TLRs), which is well below the 17% performance goal. On subgroup analysis, those receiving kissing stents had a 9-month composite primary endpoint of 3.5% (two TLRs).
Secondary endpoint data reported a primary patency rate of 96.7% at 9 months for the entire cohort. Notably, the primary patency between TASC A/B versus C/D was not significantly different at 97.4% and 95.3%, respectively. Further, 4.6% of patients had an improvement in their Rutherford classification and mean ABI improved from 0.77 to 0.97 at 9 months, with associated improvements in walking impairment scores.
Mid-term Results
Three-year data from the VBX FLEX study demonstrated continued mid-term benefit in the study population.19 Freedom from TLR on a per-lesion basis was 91.2% (18 TLRs) at 36 months. The freedom from CD-TLR estimate was 98.1% (four CD-TLRs) at 36 months. In addition, 94.6% of patients had an improvement in their Rutherford category at 9 months, and this benefit was sustained out to 3 years. The mean ± SD improvement in ABI was measured at 0.17 ± 0.26 at 3 years, with more than 85% of patients noting improved health status and walking impairment scores out to 3 years.
Sample Case of Bilateral Common Iliac Lesions
On univariate analysis, TLR was associated with women compared with men (16.4% versus 2.5%, respectively; p=0.008), the number of treated segments (1.7% for one segment versus 13.3% for two to three segments; p=0.023) and the number of devices required (2.0%, 10.1% and 21.4% for one, two and three or more devices, respectively; p=0.013).
Study Conclusion
The short- and mid-term data from the VBX FLEX study demonstrate that the VBX stent graft is a safe and durable treatment for complex AIOD. There is enduring clinical improvement and a low rate of re-intervention at 3 years.
Conclusion
Endovascular stenting has become commonplace in the aortoiliac segment. The COBEST trial is the only randomised trial to compare covered and non-covered stents in the aortoiliac segment. That trial demonstrated that, in the treatment of TASC A and B lesions, covered and non-covered stents have equivalent efficacy; however, for more complex TASC C and D lesions, covered stents have better efficacy.12 The Gore VBX stent graft offers another tool for the endovascular management of AIOD. Its unique design offers increased flexibility, high radial strength, accuracy in deployment and resistance to foreshortening. When framing the VBX stent graft in the context of the two other devices approved in the US, namely the Bard LifeStream and Atrium iCAST covered stent grafts, they all offer very similar immediate technical success and patency rates at both the 9-month and 3-year marks.16–20 However, the VBX FLEX study population had a higher proportion of TASC C and D lesions, which indicates sustained high performance for treating more advanced disease.18 The iCAST stent graft is the only covered stent graft for which long-term outcomes data are available, with a documented primary patency of 74.7% at 5 years.20 It remains to be seen how the long-term durability of the VBX stent will compare.
-
- Shu J, Santulli G. Update on peripheral artery disease: epidemiology and evidence-based facts. Atherosclerosis 2018;275:379–81.
Crossref| PubMed - Rueda CA, Nehler MR, Perry DJ, et al. Patterns of artery disease in 450 patients undergoing revascularization for critical limb ischemia: implications for clinical trial design. J Vasc Surg 2008;47:995–9.
Crossref| PubMed - Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg 2007;45(Suppl S):S5–67.
Crossref| PubMed - Society for Vascular Surgery Lower Extremity Guidelines Writing Group, Conte MS, Pomposelli FB, et al. Society for Vascular Surgery practice guidelines for atherosclerotic occlusive disease of the lower extremities: management of asymptomatic disease and claudication. J Vasc Surg 2015;61(3 Suppl):2S–41S.
Crossref| PubMed - Palmaz JC, Richter GM, Nöldge G, et al. Intraluminal Palmaz stent implantation. The first clinical case report on a balloon-expanded vascular prosthesis. Radiologe 1987;27:560–3 [in German].
PubMed - Palmaz JC, Richter GM, Noeldge G, et al. Intraluminal stents in atherosclerotic iliac artery stenosis: preliminary report of a multicenter study. Radiology 1988;168:727–31.
Crossref| PubMed - Palmaz JC, Garcia OJ, Schatz RA, et al. Placement of balloon-expandable intraluminal stents in iliac arteries: first 171 procedures. Radiology 1990;174:969–75.
Crossref| PubMed - Tetteroo E, van der Graaf Y, Bosch JL, et al. Randomised comparison of primary stent placement versus primary angioplasty followed by selective stent placement in patients with iliac-artery occlusive disease. Lancet 1998;351:1153–9.
Crossref| PubMed - AbuRahma AF, Hayes JD, Flaherty SK, et al. Primary iliac stenting versus transluminal angioplasty with selective stenting. J Vasc Surg 2007;46:965–70.
Crossref| PubMed - Ye W, Liu CW, Ricco JB, et al. Early and late outcomes of percutaneous treatment of TransAtlantic Inter-Society Consensus class C and D aorto-iliac lesions. J Vasc Surg 2011;53:1728–37.
Crossref| PubMed - Goode SD, Cleveland TJ, Gaines PA. Randomized clinical trial of stents versus angioplasty for the treatment of iliac artery occlusions (STAG trial). Br J Surg 2013;100:1148–53.
Crossref| PubMed - Mwipatayi BP, Thomas S, Wong J, et al. A comparison of covered versus bare expandable stents for the treatment of aortoiliac occlusive disease. J Vasc Surg 2010;54:1561–70.
Crossref| PubMed - Sabri SS, Choudhri A, Orgera G, et al. Outcomes of covered kissing stent placement compared with bare metal stent placement in the treatment of atherosclerotic occlusive disease at the aortic bifurcation. J Vasc Interv Radiol 2010;21:995–1003.
Crossref| PubMed - Mwipatayi BP, Sharma S, Daneshmand A, et al. Durability of the balloon-expandable covered versus bare-metal stents in the Covered versus Balloon Expandable Stent Trial (COBEST) for the treatment of aortoiliac occlusive disease. J Vasc Surg 2016;64:83–94.e1.
Crossref| PubMed - Bekken JA, Vos JA, Aarts RA, et al. DISCOVER: Dutch Iliac Stent trial: COVERed balloon-expandable versus uncovered balloon-expandable stents in the common iliac artery: study protocol for a randomized controlled trial. Trials 2012;13:215.
Crossref| PubMed - Laird JR, Zeller T, Holden A, et al. Balloon-expandable vascular covered stent in the treatment of iliac artery occlusive disease: 9-month results from the BOLSTER multicenter study. J Vasc Interv Radiol 2019;30:836–44.e1.
Crossref| PubMed - Laird JR, Loja M, Zeller T, et al. iCAST balloon-expandable covered stent for iliac artery lesions: 3-year results from the iCARUS multicenter study. J Vasc Interv Radiol 2019:30;822–9.e4.
Crossref| PubMed - Bismuth J, Gray BH, Holden A, et al. Pivotal study of a next-generation balloon-expandable stent-graft for treatment of iliac occlusive disease. J Endovasc Ther 2017;24:629–37.
Crossref| PubMed - Panneton JM, Bismuth J, Gray BH, et al. Three-year follow-up of patients with iliac occlusive disease treated with the Viabahn balloon-expandable endoprosthesis. J Endovasc Ther 2020;27:728–36.
Crossref| PubMed - Mwipatayi BP, Ouriel K, Anwari T, et al. A systematic review of covered balloon-expandable stents for treating aortoiliac occlusive disease. J Vasc Surg 2020;72:1473–86.e2.
Crossref| PubMed - GORE. https://eifu.goremedical.com/ (accessed 23 August
- Shu J, Santulli G. Update on peripheral artery disease: epidemiology and evidence-based facts. Atherosclerosis 2018;275:379–81.