Stefano Fazzini, Valerio Turriziani, Federico Francisco Pennetta, Simona Vona, Fabio Massimo Oddi, Andrea Ascoli Marchetti, Konstantinos P Donas, Arnaldo Ippoliti
|
Abstract The use of chimney technique in endovascular repair of abdominal aortic aneurysms (ChEVAR) has had a secondary role. Although it was first developed in an emergent/urgent setting, the publication of various important studies has helped overcome scepticism towards this technique in elective procedures. This paper reviews current evidence about ChEVAR, focusing on clinical results, technical notes and comparisons with other techniques. The new ChEVAR findings show favourable mid- and long-term clinical outcomes, even in elective patients. These results, comparable to those related to fenestrated endografts, have been achieved through standardisation in planning and materials. An adequate endograft oversizing associated to the right aortic neck length is fundamental to avoid ChEVAR-related complications, such as type 1a endoleaks. These data indicate that ChEVAR, compared to other complex endovascular treatments, has comparable outcomes along with features that could make it an essential option in every clinical setting. Keywords Chimney endovascular aortic repair, chimney graft, juxtarenal abdominal aortic aneurysm, pararenal abdominal aortic aneurysm, endovascular aortic repair, fenestrated endovascular aortic repair, planning Disclosure: KPD is on the Vascular & Endovascular Review editorial board; this did not influence peer review. All other authors have no conflicts of interest to declare. Received:Accepted: Published online: Correspondence Details: Stefano Fazzini, Vascular Surgery Unit, Biomedicine and Prevention Department, Tor Vergata University, Viale Oxford 81, 00133 Rome, Italy. Open Access: This work is open access under the CC-BY-NC 4.0 License which allows users to copy, redistribute and make derivative works for non-commercial purposes, provided the original work is cited correctly.
|
In the last decade, the use of chimney technique has become an alternative solution for the endovascular treatment of juxtarenal aneurysms (j-AAA) and, in particular cases, pararenal aneurysms (p-AAA). Chimney endovascular aortic repair (ChEVAR) has emerged as an off-label procedure in cases of unintended renal artery coverage. The use of off-the-shelf devices has led to a broad application of this technique, mainly in urgent conditions of treatment. However, this indication has been limited by the lack of profound scientific clinical evidence due to wide heterogeneous data regarding device combinations and the degree of oversizing. Scepticism has subsided in recent years after the publication of landmark studies (Table 1), which is now leading to a standardisation in the use of this technique. In this paper, we present a review of current evidence on ChEVAR, focusing on clinical results, technical notes, and comparisons with other techniques.
Indications and Main Clinical Data
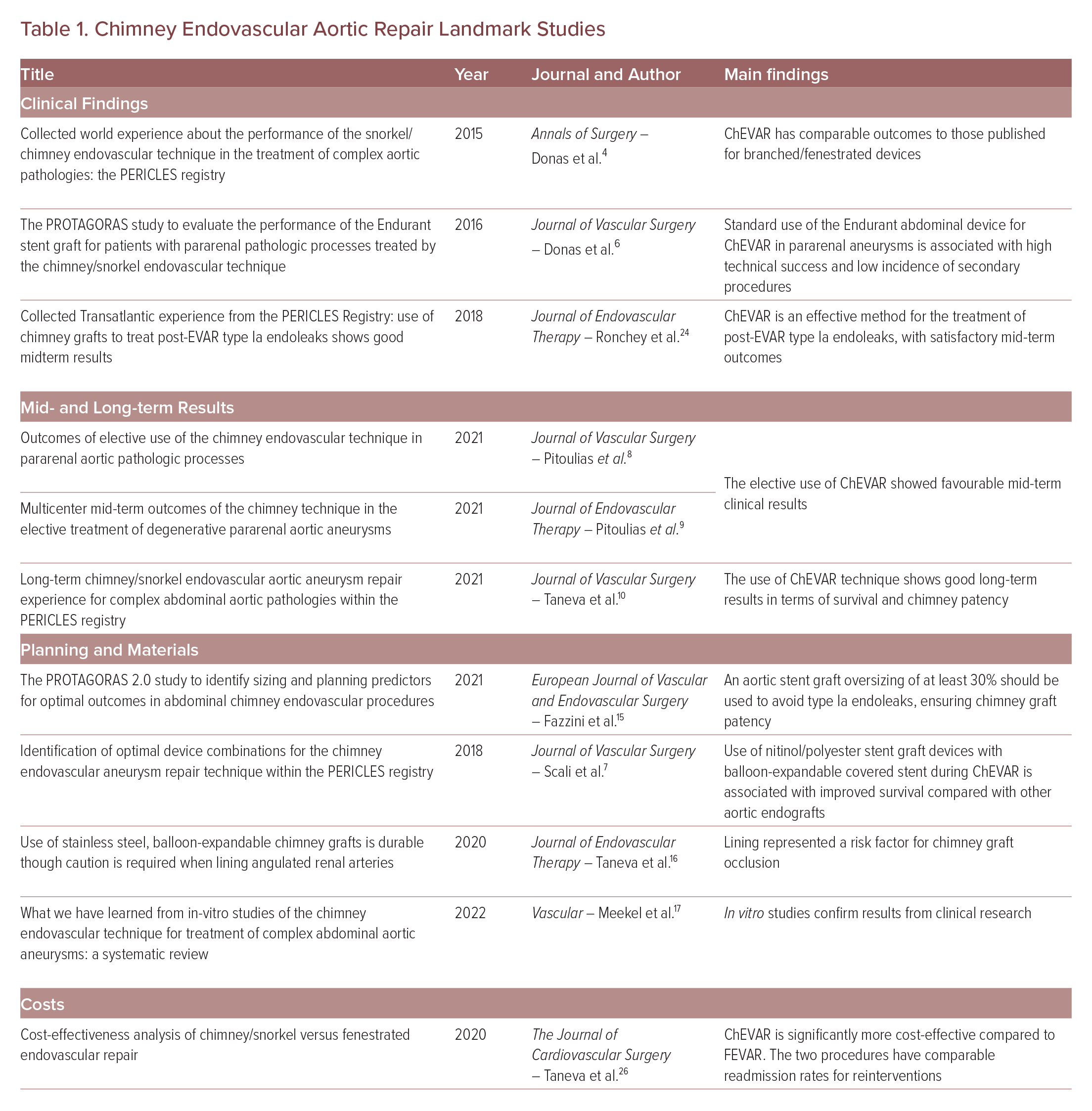
ChEVAR has been developed primarily in an emergent/urgent setting (Figure 1), where it could still be considered the first-line option for the treatment of ruptured or symptomatic j-AAAs and p-AAAs, mostly due to its off-the-shelf availability.1–3 The conception of this technique changed in 2015 with the publication of clinical results from the PERICLES registry, which involved 517 patients from 13 international centres, showing a technical success of 97.1%, an estimated primary patency of 94.1% and a 30-day mortality of 4.9%.4 However, the most interesting finding of the PERICLES registry data was that ChEVAR clinical outcomes were comparable to those already published for fenestrated endovascular aortic repair (FEVAR). One of the main limitations of this technique could be the use of heterogeneous endograft/chimney stent combinations with influence on the outcomes.
As suggested in a multicentre French national retrospective study, the use of various device/stent combinations leads to non-optimal clinical outcomes: a polyester/stainless steel endograft is associated with lower 1- and 3-year survival rates compared to polyester/nitinol endografts.5
The need for ChEVAR standardisation was first investigated in 2016 by Donas et al. in the PROTAGORAS study, which evaluated the performance of the Endurant stent graft (Medtronic), demonstrating high technical success with a low incidence of secondary interventions.6 The identification of an ideal device combination for ChEVAR has also been investigated by Scali et al., who analysed the PERICLES registry outcomes and established that the combination of nitinol/polyester stent graft devices (such as the Endurant stent graft) with balloon-expandable covered stents (BECS) is associated with improved survival compared with other endografts.7 This combination had the best clinical outcomes in terms of type 1a endoleaks and chimney graft (CG) occlusion; nitinol endograft endoskeleton and BECS allow proper conformability and radial strength, respectively.
Mid-term and Long-term Results
Pitoulias et al. presented the results of ChEVAR single-centre experience in an elective setting using a single aortic device (Endurant stent graft), demonstrating that a standardised protocol leads to favourable mid-term clinical outcomes comparable to those published for fenestrated grafts: freedom from persistent type 1a endoleak at 3 years was 95.3%, with an overall ChEVAR-related mortality of 1.8%.8 Similar results have been observed in a multicentre study that analysed ChEVAR use in elective patients with p-AAA (freedom from type 1a endoleak at 3 years 93%, overall ChEVAR-related mortality 2.2%).9
The promising results seen in ChEVAR have been confirmed in a recently published study that analysed long-term clinical conditions of patients included in the PERICLES registry. ChEVAR showed favourable long-term results, with a CG patency of 92% and more than half of the patients surviving more than 5 years after the procedure (66.1%).10 Similar long-term outcomes have been observed in various studies of FEVAR in j-AAAs, showing comparable survival rates at 5 years.11,12
The accumulation of data now clearly indicates that ChEVAR can have an important role in the routine treatment of abdominal aortic aneurysms (AAAs), particularly in cases of j-AAA where the number of CGs is limited to one or two stents.13 Moreover, thanks to proven device combination (Endurant II/IIs stent graft and Advanta V12/iCast [Getinge]), Medtronic recently announced CE marking for its Radiant™ balloon-expandable covered stent leveraging the Advanta V12 design. The Radiant-covered stent is the first and currently the only parallel graft indicated for use in ChEVAR with the Endurant II/IIs. This new device combination, named EnChEVAR by the company, represents a standardised, fully on-label, off-the-shelf solution for short-neck and j-AAA.14
Technical Notes: Planning and Sizing
Planning has a fundamental role in ChEVAR in avoiding device-related complications, such as type 1a endoleaks which are widely considered the Achilles heel of this technique.
Very recently, the PROTAGORAS 2.0 study analysed a single chimney-graft combination (Endurant and BECS Advanta V12/iCast).15 This study provides a clinical trial application analysis of predictors of adequate preoperative planning and sizing, concluding that the most important parameter for ChEVAR planning is aortic stent graft oversizing. According to this study, an oversizing of at least 30% is recommended to avoid persistent type 1a endoleaks without compromising CG patency. A higher oversizing rate of at least 35% is recommended in double chimney and/or challenging neck anatomies.
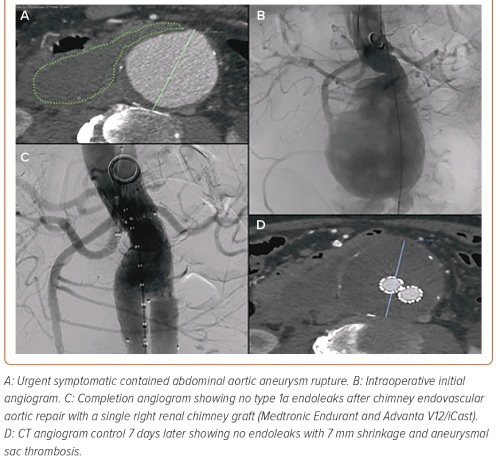
Contrary to general belief, while this study recommended a total neck length >20 mm, that length did not seem to guarantee sealing without adequate oversizing. As this parameter depends on aortic neck diameter and endograft sizing, an aortic neck >27–28 mm should not be treated by ChEVAR. PROTAGORAS 2.0 introduced a new composite parameter, the L-OS, as a combination of total neck length and oversizing, to evaluate a balance between neck length and oversizing: an L-OS range of 55–65 was strongly correlated to freedom from persistent 1a endoleaks and primary CG patency. The two main contraindications for this technique (as observed in long-term results of the PERICLES registry and PROTAGORAS 2.0) are the wide neck due to inadequate endograft oversizing, and the pararenal neck, given the absence of any infrarenal sealing zone.10,15 While there is no solution to treat wide necks using abdominal devices, accurate planning and a higher rate of oversizing could be the best treatment of pararenal necks for ChEVAR. Based on European guidelines and instructions for use (at least 2 mm of infrarenal neck, total neck length of 15 mm, infrarenal angle <60°) with the Endurant stent graft CE marking, the main indication for ChEVAR should be the treatment of j-AAA. The most recently published data supports these indications by focusing on accurate sizing (oversizing >30%, total neck length >20 mm) and adapting to a wider range of anatomies (pararenal neck, very angulated necks [Figure 2]).
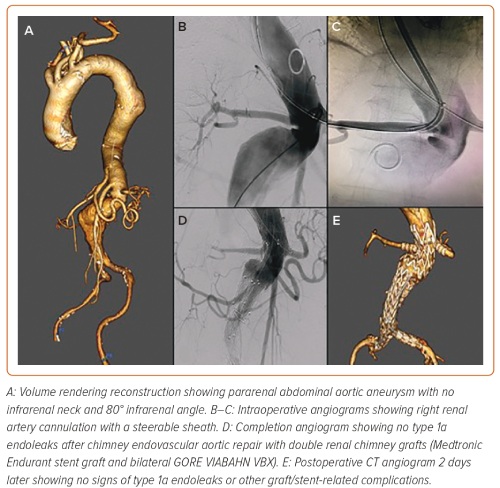
Careful planning with an appropriate choice of materials is also important to avoid CG occlusion. A recent study that evaluated 116 patients who underwent ChEVAR found that, while the use of BECS had proven long-term results, CG lining was strongly correlated with chimney occlusion. CG lining is performed with the additional deployment of a flexible bare nitinol stent to improve the transition of a CG in an angulated artery.16 This highlights the importance of proper preoperative planning, fundamental to optimising CG positioning and length, thus reducing the need for adjunctive stent deployment. The CGs allow a more proximal sealing zone for the endograft and unlike BEVAR, there is no need for longer sealing zone in target vessels.
Various in vitro studies have evaluated the performance of different device combinations and the influence of oversizing and sealing length on gutter behaviour. A recent review of these studies found results similar to those observed in clinical research: 30% oversizing and use of BECS are associated with lower rates of gutter endoleak and CG occlusion, respectively.17 In vitro studies can help improve our knowledge of different applications of the chimney technique. Nevertheless, the role of future research in evaluating the performance of different device combinations remains crucial in clinical practice.
Complications and Limitations
Several studies underline that ChEVAR and FEVAR can have comparable outcomes in terms of feasibility, safety and efficacy in elective patients. The major concern about ChEVAR is the rate of gutter endoleaks (type 1a). While an early gutter endoleak can be seen in a significant number of ChEVAR procedures, it has been observed that most of these cases can have a spontaneous resolution.18
Although ChEVAR has significant rates of type 1a endoleak, it does not seem to affect mortality. In a series of elective ChEVAR in p-AAAs by Pitoulias et al., the 1a endoleak rate was 3.6% with a 30-day mortality rate of 1.8%, comparable to data from similar patients treated with FEVAR (2%).8,19 As mentioned, an oversize of >30% has been associated with significantly improved freedom from type 1a endoleak-related reinterventions: in the PROTAGORAS 2.0 study, patients with persistent Ia endoleaks had a median oversize of 18%. Similar results were also observed in large multicentre studies where adequate planning and j-AAAs are associated with lower rates of type 1a endoleak.5
Availability and Versatility
An important feature of ChEVAR is the availability of off-the-shelf devices. While aortic endografts used for other complex endovascular treatments (such as fenestrated or branched grafts) may not be available everywhere, especially in developing countries, ChEVAR can be performed with widely available devices.20
In some cases, such as larger and/or symptomatic aneurysms, the 6–8-week period required to manufacture custom-made devices may be too long. For these patients, other off-the-shelf branched endografts (t-Branch® [Cook Medical], E-nside [Artivion]) could be adopted; nonetheless, this would increase the number of treated visceral vessels and the risk of spinal cord ischaemia by covering a longer aortic segment.
Promising results have emerged recently from the use of physician-modified endografts (PMEG) both in urgent and elective patients: however, there is scarce data regarding mid- and long-term follow-up, so further studies are needed to assess the role of this technique.21,22
Compared to other complex endovascular techniques, ChEVAR is also important for its versatility. It can be extremely useful, using low-profile abdominal aortic devices, in cases of hostile iliac access, especially in women. Torsello et al. presented an analysis that found no significant difference between men and women after ChEVAR, while the female sex had been previously reported to be a risk factor for worse outcomes after complex endovascular and open aortic repair.23
Another important indication for ChEVAR could be the treatment of type 1a endoleak in previous EVAR, given the option to seal the leak by using aortic cuffs and a single or double chimney. In addition, in these cases, the waiting time for custom-made devices could be a contraindication.24 Data from the literature confirm that patency of target vessels is comparable between ChEVAR and fenestrated grafts, especially when considering elective cases.8 Over time, custom-made devices could have bridging stent graft instability, with aortic remodelling in branched stent grafts (BEVAR) in larger aneurysms but also in fenestrated grafts, with graft migration and rotation that could be at risk, especially for scallops.25 Moreover, reintervention in cases of fenestrated graft or a second procedure, such as thoracic graft deployment, could be at risk of stent compression and/or dislocation caused by the presence of flared stents inside the grafts. Furthermore, recent research from Taneva et al. observed that ChEVAR is significantly more cost-effective than FEVAR.26 The two procedures have comparable outcomes and hospital readmission rates, but ChEVAR has significantly lower costs both for primary procedure and secondary reintervention.
Conclusion
Data indicates that ChEVAR is a safe and valid option for urgent and elective treatment of AAAs with short aortic neck. The inclusion of ChEVAR in the 2019 European Society for Vascular Surgery (ESVS) guidelines is an important example of the increasing role that this technique has in the treatment of complex aortic pathologies.3 Although there are still concerns about its limits, especially for type 1a endoleak, recent data demonstrate favourable long-term outcomes. Compared to other complex endovascular procedures, ChEVAR has some important features that could make it the preferred option for the treatment of j-AAAs and p-AAAs, such as standardised device combination and sizing, urgent setting indications, feasibility in hostile iliac access, use of off-the-shelf devices available worldwide and lower costs. We trust that a standardisation of this technique based on planning and device selection could help improve clinical outcomes.
- Jernigan EG, Nguyen Tran N, Qato K, et al. Outcomes of chimney/snorkel endovascular repair for symptomatic and ruptured abdominal aortic aneurysms. J Vasc Surg 2021;74:1117–24.
Crossref | PubMed - Keschenau PR, Beropoulis E, Gombert A, et al. The role of surgical and total endovascular techniques in the treatment of ruptured juxtarenal aortic aneurysms. Vasa 2021;50:356–62.
Crossref | PubMed - Wanhainen A, Verzini F, Van Herzeele I, et al. Editor’s choice – European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg 2019;57:8–93.
Crossref | PubMed - Donas KP, Lee JT, Lachat M, et al. Collected world experience about the performance of the snorkel/chimney endovascular technique in the treatment of complex aortic pathologies: the PERICLES registry. Ann Surg 2015;262:546–53.
Crossref | PubMed - Touma J, Caradu C, Sylvestre R, et al. Multicentre experience with the chimney technique for abdominal aortic aneurysms in French university hospitals. Eur J Vasc Endovasc Surg 2020;59:776–84.
Crossref | PubMed - Donas KP, Torsello GB, Piccoli G, et al. The PROTAGORAS study to evaluate the performance of the Endurant stent graft for patients with pararenal pathologic processes treated by the chimney/snorkel endovascular technique. J Vasc Surg 2016;63:17.
Crossref | PubMed - Scali ST, Beck AW, Torsello G, et al. Identification of optimal device combinations for the chimney endovascular aneurysm repair technique within the PERICLES registry. J Vasc Surg 2018;68:24–35.
Crossref | PubMed - Pitoulias GA, Torsello G, Austermann M, et al. Outcomes of elective use of the chimney endovascular technique in pararenal aortic pathologic processes. J Vasc Surg 2021;73:433–42.
Crossref | PubMed - Pitoulias GA, Fazzini S, Donas KP, et al. Multicenter mid-term outcomes of the chimney technique in the elective treatment of degenerative pararenal aortic aneurysms. J Endovasc Ther 2022;29:226–39.
Crossref | PubMed - Taneva GT, Lee JT, Tran K, et al. Long-term chimney/snorkel endovascular aortic aneurysm repair experience for complex abdominal aortic pathologies within the PERICLES registry. J Vasc Surg 2021;73:1942–9.
Crossref | PubMed - Gallitto E, Faggioli G, Giordano J, et al. Early and mid-term efficacy of fenestrated endograft in the treatment of juxta-renal aortic aneurysms. Ann Vasc Surg 2020;66:132–41.
Crossref | PubMed - Sveinsson M, Sonesson B, Kristmundsson T, et al. Long-term outcomes after fenestrated endovascular aortic repair for juxtarenal aortic aneurysms. J Vasc Surg 2022;75:1164–70.
Crossref | PubMed - Taneva GT, Criado FJ, Torsello G, et al. Results of chimney endovascular aneurysm repair as used in the PERICLES registry to treat patients with suprarenal aortic pathologies. J Vasc Surg 2020;71:1521–7.
Crossref | PubMed - Medtronic. EnChEVAR: elevating ChEVAR therapy. 2022. (accessed 13 February 2023).
- Fazzini S, Martinelli O, Torsello G, et al. The PROTAGORAS 2.0 study to identify sizing and planning predictors for optimal outcomes in abdominal chimney endovascular procedures. Eur J Vasc Endovasc Surg 2021;61:591–602.(accessed 13 February 2023)
Crossref | PubMed - Taneva GT, Fazzini S, Pipitone MD, et al. Use of stainless-steel, balloon-expandable chimney grafts is durable though caution is required when lining angulated renal arteries.
J Endovasc Ther 2020;27:902–9.
Crossref | PubMed - Meekel JP, Tran BL, van Schaik TG, et al. What we have learned from in-vitro studies of the chimney endovascular technique for treatment of complex abdominal aortic aneurysms: a systematic review. Vascular 2022.
Crossref | PubMed - Ullery BW, Tran K, Itoga NK, et al. Natural history of gutter-related type Ia endoleaks after snorkel/chimney endovascular aneurysm repair. J Vasc Surg 2017;65:981–90.
Crossref | PubMed - Wang SK, Gutwein AR, Gupta AK, et al. Institutional experience with the Zenith Fenestrated aortic stent graft. JVasc Surg 2018;68:331–6.
Crossref | PubMed - Nugroho N, Usai MV, Fazzini S, Nugroho NT. How to deal with the Achilles heel of the chimney endovascular technique for complex aortic pathologies. Journal of the Indonesian Society for Vascular and Endovascular Surgery 2020;1:i–ii.
Crossref | PubMed - Koleilat I, Nussenblatt B, Freidmann P, et al. Physician-modified endografts versus chimney/snorkel for ruptured and symptomatic juxtarenal and paravisceral aneurysms in the vascular quality initiative. Ann Vasc Surg 2021;82:249–57.
Crossref | PubMed - Gouveia E Melo R, Fernández Prendes C, Caldeira D, et al. Systematic review and meta-analysis of physician modified endografts for treatment of thoraco-abdominal and complex abdominal aortic aneurysms. Eur J Vasc Endovasc Surg 2022;64:188–99.
Crossref | PubMed - Torsello G, Usai MV, Scali S, et al. Gender-related outcomes of chimney EVAR within the PERICLES registry. Vascular 2018;26:641–6.
Crossref | PubMed - Ronchey S, Fazzini S, Scali S, et al. Collected Transatlantic experience from the PERICLES Registry: use of chimney grafts to treat post-EVAR type Ia endoleaks shows good midterm results. J Endovasc Ther 2018;25:492–8.
Crossref | PubMed - Fazzini S, Torsello G, Austermann M, et al. Aortic endograft and bridging stent-graft remodeling after branched endovascular aortic repair. Vascular 2021;29:808–16.
Crossref | PubMed - Taneva GT, Donas KP, Pitoulias GA, et al. Cost-effectiveness analysis of chimney/snorkel versus fenestrated endovascular repair for high-risk patients with complex abdominal aortic pathologies. J Cardiovasc Surg (Torino) 2020;61:18–23.
Crossref | PubMed